As some one planning on specializing in reproductive medicine, I actually don’t like the term “infertile,” or the phrase that we often hear that some one is “struggling with infertility.” It’s very rare for a woman to be either 100% fertile, or 100% infertile, which …
Sleep Deprivation in Mommyhood The Relationship between Breastfeeding, Sleep deprivation, and Depression Realistic Expectations after Delivery The idealistic expectations fed to mommy-t0-bes from the social media world can cause legitimate anxiety. Even well meaning friends can paint unrealistic pictures of what your recovery and postpartum …
Labor after 20 weeks and prior to 37 weeks is considered preterm.1 One in every ten babies is born premature.2 Further categories of prematurity are based on gestational age as listed below.3 –Less than 28 weeks = extremely preterm –28 weeks to 32 weeks = very preterm –32 weeks to 37 weeks = moderate to late preterm
Problems Associated With Premature Delivery
Understandably, the earlier a baby is born, the more likely he or she will have greater health complications. While two of the largest problems associated with prematurity deal with the baby’s brain and lungs, the rest of the body may also be affected. This includes the baby’s immune system, eyes, ears, intestines, and even issues with their teeth growth.4These issues can be scary and parents customarily want to do anything and everything they can to best help their baby. One thing parents can do is to offer their baby human breast milk, “breastfeeding benefits preterm infants from a nutritional, gastrointestinal, immunological, developmental, and psychological perspective.”5
Why Breastfeed a Premature Baby?
*Information in this area is summarized from from the meta analysis, “A Review of the Literature Examining the Benefits and Challenges, Incidence and Duration, and Barriers to Breastfeeding in Preterm Infants”6
Whey proteins from human milk are easier to digest and cause rapid gastric emptying, which is beneficial for the preterm infants’ gastrointestinal system.
The hormones, peptides, amino acids, and glycoproteins may also assist mature the small intestine.
Human breast milk contains a-lactalbumin, lactoferrin, lysozyme, and secretory immunoglobulin A, these aid to build the immunity of the baby giving “optimal immune defense.” These also aid in better digestion.
Human breast milk contains lactose and oligosaccharides which are carbohydrates that aid in improving absorption of minerals and increase the beneficial bacteria in the intestines which help prevent against Necrotizing enterocolitis (NEC).
Lipids in breast milk and the presence of bile salt-stimulated lipase allow the premature baby to absorb greater amounts of fat (as long as the milk is unprocessed).
Human milk contains long-chain fatty acids that aid in cognition and vision growth.
One study found that preterm infants fed human milk versus formula had a “reduction in the development of allergic symptoms.”
Psychological benefit for the mother. Mothers report feelings of attachment, empowerment, and confidence when supplying their baby with their own breast milk.
The breastfeeding mother produces sIgA antibodies when exposed to foreign antigens. The infant receives these antibodies through the breast milk creating a “passive immunity” to the baby’s immediate environment.
Premature Breast Milk vs. Mature Breast Milk
For the first couple of weeks, mothers of premature babies develop breast milk that is unique to meet their premature baby’s needs. The premature milk is higher in proteins, minerals including salt, and has fats that are easier to digest.7
Challenges Associated with Breastfeeding a Premature Baby
Although breastfeeding greatly benefits premature babies, there are specific challenges that affect a premature baby’s ability to breastfeed. The baby may not be physiologically stable to be at the mother’s breast and may only be able to be fed through a tube (gavage feedings). Later on when the infant is stable, breastfeeding may be difficult due to transitioning from gavage feedings to suckling on the breast. The mother may also have a difficult time creating and maintaining a milk supply for her preterm baby. Furthermore, dependent on the baby’s weight and gestation, the baby may need more nutrients in addition to the human breast milk.8Even though human milk is recommended as the best milk for all infants including preterm, “no naturally occurring human milk can meet, without fortification, the increased nutrient requirements of very-low birth weight infants”9 A “very-low birth weight infant” includes any baby born less than 1.5kg or 3.13lbs.10
Tricks to Combat The Challenges of Breastfeeding a Premature Baby
Initiating Lactation (secretion of milk) through Pumping
If your baby is not physiologically stable, he or she will not be able to directly breastfeed and early initiation of breast pumping is vital. The breast pump should create a “milking action and not simply be a sucking device.” Pumping should be at regular intervals, aiming to pump “at least six to eight times a day.” Breast Pumping throughout the night is also needed, if breast fullness is noted upon awakening, you should pump more frequently, if trying to increase your milk supply. You should also not sleep for longer than four to five hours without pumping for at least the first couple of weeks.11
Maintaining a Milk Supply
Inadequate milk supply is the number one concern for mothers feeding their preterm infants. Breast milk supply runs by demand and due to the immaturity, weakness, and ineffectiveness of a preterm baby’s suck, the mother’s milk supply can be hindered. In one study, optimal milk production was associated with five or more milk expressions per day with pumping durations equaling more than 100 minutes per day!12
Quit Smoking
Breastfeeding is not contraindicated in cigarette smoking mothers.13 But, if you are smoking, please try to quit! Not only does second hand smoke harm your preterm baby, it also drastically decreases your breast milk supply.14 For help to quit smoking see, “4 Steps to Quit Smoking”.
Sequential Versus Simultaneous Breast Pumping
Pumping both breasts at the same time will cause you to express breast milk in a shorter amount of time as well as have an increase in prolactin levels.15 While two studies in 2001 have showed no change in the overall volume of milk produced,16 Jones states that their study published in 2001 “clearly shows that simultaneous pumping, with or without massage, is more effective than single pumping in producing an increased volume of milk.”17
Since then, a 2012 study has been published to support Jones. Although the study was only completed on mothers with term babies, their findings showed that simultaneous breast pumping is advantageous over sequential due an increase amount of milk in a shorter amount of time. They also found that simultaneous breast pumping produced milk with a higher cream content than sequential pumping thus giving baby more energy.18
Breast Massage
Breast massaging prior to pumping and during has shown to assist and increase your milk flow. To breast massage, gently use your fingertips to make circular motions starting at the outer edges of your breast working your way towards the nipple.
When an unclothed baby is placed skin to skin with its mother (kangaroo care) it has shown to increase and sustain the mother’s milk supply and in return facilitates infant growth. Kangaroo care also assists the baby to be more comfortable at the breast a more competent breastfeeder. When your baby is stable to do kangaroo care, nurses in the neonatal intensive care unit (NICU) will assist you with this. Skin to skin care has also shown to help regulate the baby’s temperature, heart rate, and assist in the infant’s sleep organization. This is important because it helps to decrease your baby’s “energy expenditure.”19
Decrease Stress
Stress and fatigue have shown to have a decrease in milk production.20 Having a premature baby in NICU is extremely stressful and exhausting. Find a way to to manage your emotions if that is a daily walk outside, journaling, bath or channeling your spiritual side. Do what works for you.
Rooming In
Find out what your hospital offers regarding visiting hours in the NICU as well as “rooming in.” Moms who stay with their infants as much as possible have a greater milk supply, breastfeed longer, and are more likely to breastfeed exclusively.21
Food, Herbs, & Medications Used to Increase Milk Production
Galactogogues are substances that promote lactation. Many foods and herbs are used for these properties. Here is list from the article “Selection and Use of Galactogogues” that are commonly used:
Glactogogues medications may be used to increase a mother’s milk supply after non-pharmacologic interventions have been tried. The most common prescriptions include Domperidone, Metoclopramide, Metformin, and Oxytocin. Although, Food and Drug Administration (FDA) in 2004 issued a recommendation against the use of domperidone due to safety concerns.22
Non-Nutritive Sucking
Non-nutritive sucking assists the development of the baby’s ability to suck, it also increases the baby’s saliva that allows the baby to practice swallowing aiding in the digestion of the tube feedings.23
Goal Setting
One study published by The Journal of Human Lactation in 2015 showed that making a goal that is “time specific” increased the likelihood of the mother and baby to be breastfeeding at time of discharge. “The ultimate goal is for mothers to provide exclusive human milk feedings for the first 6 months of age, with continued human milk feeding along with other foods until at least 1 year of age.”24
Feed Directly at The Breast Before Utilizing The Bottle
Infants who receive their first “oral feeding” as direct breastfeeding versus bottle feeding are more likely to directly breastfeed more often and to be breastfeeding at discharge. Also, infants who are fed directly at the breast are shown to receive breast milk for longer versus babies who receive breastmilk from the bottle.25
Donor Milk
If you are not able to supply your preterm baby with enough or any breastmilk for multiple reasons, donor milk can be an adequate substitute. Both fresh and banked human milk have shown to have specific benefits for preterm infants. Similarly to your own fresh breast milk, donor milk may also need to be fortified if your baby has extra caloric needs. One study did find that donor milk has a slightly lower caloric value of 19kcal/oz versus the generally accepted caloric amount of fresh breast milk of 20kcal/oz. Very low birth weight infants are in need of approximately 120kcal a day. If you are interested, ask your neonatologist or nurses if donor milk is an option for you.26
Support
Practice breastfeeding while at the hospital utilizing a lactation consultant to best learn your baby’s feeding cues, holding techniques, and latching strategies.27 When women participate in a breastfeeding support group it has shown that they breastfeed for a longer duration. Ask your NICU nurses what support groups they can offer including WIC clinics, lactation consultants, breast-pump rentals, or even look in your local area for lay groups.
* Like any other article of mine, this information should not supersede or replace any information given to you by your own NICU nurses or neonatologist. I hope you find this helpful in an intense time and my heart is with you!
18. DK, Prime, Garbin CP, Hartmann PE, and Kent JC. “Simultaneous Breast Expression in Breastfeeding Women Is More Efficacious than Sequential Breast Expression.”Breastfeeding Medicine : The Official Journal of the Academy of Breastfeeding Medicine. Mary Ann Liebert Inc., 6 Nov. 2012. Web.
19. Cartwright, Joanna, Teresa Atz, Susan Newman, Martina Mueller, and Jill Radtke Demirci. “An Integrative Review of Interventions to Promote Breastfeeding in the Late Preterm Infant.”Journal of Obstetric, Gynecologic & Neonatal Nursing (2017): Web.
21. Cartwright, Joanna, Teresa Atz, Susan Newman, Martina Mueller, and Jill Radtke Demirci. “An Integrative Review of Interventions to Promote Breastfeeding in the Late Preterm Infant.”Journal of Obstetric, Gynecologic & Neonatal Nursing (2017): Web.
22. Nice, Frank J., BS, MS, MPA, DPA. “Selection and Use of Galactogogues.” ICAN, Aug. 2015. Web.
24. Briere, Carrie-Ellen, Jacqueline M. Mcgrath, Xiaomei Cong, Elizabeth Brownell, and Regina Cusson. “Direct-Breastfeeding Premature Infants in the Neonatal Intensive Care Unit.”Journal of Human Lactation 31.3 (2015): 386-92. Web.
26.Briere, Carrie-Ellen, Jacqueline M. Mcgrath, Xiaomei Cong, Elizabeth Brownell, and Regina Cusson. “Direct-Breastfeeding Premature Infants in the Neonatal Intensive Care Unit.”Journal of Human Lactation 31.3 (2015): 386-92. Web.
27.Briere, Carrie-Ellen, Jacqueline M. Mcgrath, Xiaomei Cong, Elizabeth Brownell, and Regina Cusson. “Direct-Breastfeeding Premature Infants in the Neonatal Intensive Care Unit.”Journal of Human Lactation 31.3 (2015): 386-92. Web.
With each stage of your newborn’s life you may need to adjust your nursing techniques. Newborns tend to be lazy or sleepy, while infants tend to be distracted by noises and movements. Both create a unique challenge for breastfeeding. How Do I get My Newborn …
Nipples are like feet. Besides the fact that they like to be covered in the day and free in the bed, they come in many shapes and forms; large, small, flat, pointy, and even inverted. They both serve fundamental purposes– walking and feeding. Feet can …
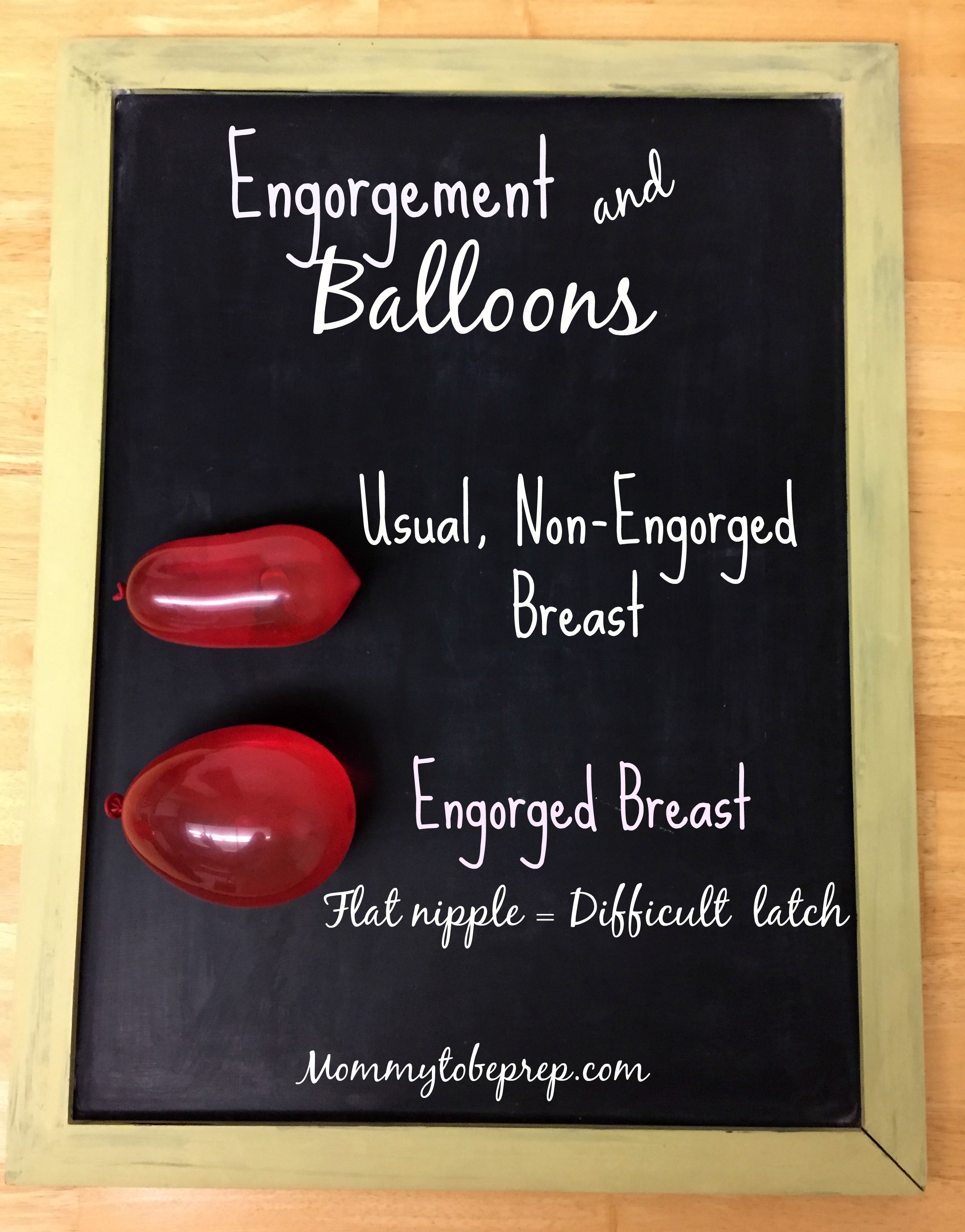
It is normal for your breasts to become more full during the second to sixth day after delivery due to your mature milk coming in. The increase in volume of milk, as well as the additional blood and fluid traveling to your breasts will give you a full sensation. Some women hardly notice, while others feel like Dolly Parton, but a sour Dolly Parton, refusing hugs at all costs! Usually this fullness will dissipate in 12-48 hours when treated correctly, if not, contact your physician.
How to Prevent & Treat Engorgement?
Ensure your baby’s latch is correct! Utilize a lactation consultant early on! If you find that you are engorged and that your nipples have become flat due to the pressure in your breasts, latching may be even more difficult. Picture yourself trying to latch hold of these water balloons with your own mouth, without the use of your own hands! You can now imagine the frustration your poor baby may experience when dealing with engorged breasts! Reverse Pressure Softening or expressing breast milk prior to nursing may soften the breasts for an easier latch. If you are unable to get your baby latched with these tricks, or your baby is not having enough wet or dirty diapers, contact your doctor.
Breastfeed frequently and on cue. If you are infected, try to breastfeed on the infected side first. La Leche League recommends, “if your baby sleeps more than two to three hours during the day or four hours at night, wake him to nurse.”
Do not switch your baby to your other breast until the baby shows signs of being completed (falling a sleep, or takes themselves off the breast independently).
If your baby is not able to nurse at the breast, but you are planning on breastfeeding, pump or self-express during the times your baby would normally be feeding.
Apply warm compresses to assist in milk let down.Lil Buds work perfect for this situation! Place them in the microwave for just 10 seconds and then on the breast (See my IG GIVEAWAY for these lavender aromatherapy breast comfort packs!) Cold compresses can also be used between feedings to decrease the pain and swelling. Lil Buds also works for this by storing the comfort packs in the freezer before use.
Gently massage the affected area using your fingers in a circular motion moving towards the nipple (this works great in a warm shower).
You thought cabbage leaves were just a myth for giving relief for engorgement? It is not! After washing, use the inner leaves and break a part the hard vein. Place inside your bra at room temperature or cold from the refrigerator. Change the leaves every couple of hours or if wilted, and of course do not continue if an allergy manifests. There are speculations, but it is not proven if it is the coolness of the cabbage leaves, or an innate property of cabbage itself that creates relief for the mother.
If engorgement is not treated properly, it may lead to acute mastitis…
Remember when Mrs. Doubtfire is making dinner for his family and it all goes to disaster? Especially when his breasts catch on fire, “This hollandaise smells like burnt rubber!” Okay how can you not bust up laughing when watching that movie!? Mastitis is a breast infection that feels something similar to your breast catching on fire! The symptoms include flu like symptoms, tenderness, warmth, redness, and usually is just in one breast.
How to Prevent and Treat Mastitis?
Call your Obstetrician as soon as possible if you develop a fever for longer than 24 hours, if you find pus or blood in your breast milk, if both breasts feel infected, if you have red streaks near the area, or if the symptoms come suddenly and are severe.
To best prevent mastitis you must know the most common causes, which include:
Plugged Ducts
Missed feedings, abrupt weaning, an incorrect latch, or use of artificial nipples can cause plugged ducts as well as pressure on your breasts. This includes, wearing restrictive clothing or sleeping on your stomach.
Continue to breastfeed on both sides using a variety of positions, this will encourage milk flow.
Do not stop breastfeeding as this could make the situation worse. If your baby is reluctant to breastfeed on the infected breast, self-express or pump to keep the breast soft.
Wear a comfortable supportive bra that is not too tight.
Warm compresses as well as massage, as mentioned above.
A break in the skin creates a route for infection to enter. Keep your nipples moisturized and work on that latch!Use a nipple moisturizer such as Lanolin (you may get free samples at Dr. office or hospital) or APNO (All Purpose Nipple Ointment), which you will need a prescription for and is best to get at a compound pharmacy.
A Mother with a Low Resistance to Infection
Excessive blood loss from delivery can cause you to be anemic which increases your risk for infection. Get your iron supplement!
Cigarette smoking is a double whammy because it puts a mother more at risk for plugged ducts and infection. See my post “4 Steps To Quit Smoking While Pregnant” If smoking, stop smoking.
Stress, not eating well, and a lack of sleep can all contribute to a less efficient immune system. Put your feet up and rest in bed! Mastitis is often the first sign that you are over working yourself!
Along with these other treatments, your provider may choose to put you on an antibiotic.
Most Mamas can make plenty of milk for their baby or babies. Make sure low milk supply is in fact something you are experiencing before you start treating it! Milk supply is a balancing act and overcorrecting a low supply can land you in the …
The down side of having a spitty and gassy baby is that the laundry load increases exponentially and you may indefinitely smell of sour milk. On the plus side, you always have a baby to blame postpartum toots on (I mean flatulence). In all reality, …
This is when you and your baby have been breastfeeding for a while, but now your baby is getting fussy at the breast or refusing the breast all together. FRUSTRATION would be a normal emotion at this point! It is important to know that this “strike” does not necessarily mean that your baby is ready to wean, but it could be your baby is trying to tell you something.
Reasons Your Baby may go on Strike & How to Cope
Pain
Your baby may not want to breastfeed due to pain. Possibilities include mouth pain “from teething, a fungal infection like thrush, or a cold sore” (Womenshealth.gov). An ear infection can also cause an infant to have pain while sucking. Keep in mind breastfed babies are less likely to have ear infections than formula fed babies, but it still is possible! (La Leche League International) Recent vaccination may also cause pain at the injection site making your baby uncomfortable in a particular breastfeeding position.
Consult with your pediatrician if you believe your baby is sick. Try switching breastfeeding positions to help ease any pain.
Frustration
Your baby may be getting frustrated that he or she is not getting the right amount of milk (see Over Production of Milk Supply and Too Little Milk Supply).
Airway
If your baby is congested, it will make breathing while breastfeeding more difficult. (Womenshealth.gov) Use a nasal aspirator or bulb syringe to clear your baby’s nares.
Emotional Stress
Babies are highly sensitive to their family’s emotions and to their surroundings. Your baby may choose not to eat if they are over stimulated or stressed. Try to calm your own emotions by taking a few deep breaths. If you are still feeling anxious, overwhelmed, or tense, you may need to put your baby in a safe place such as the crib and step away for a few minutes to cool yourself.
To decrease stimulation for the baby while breastfeeding, try feeding in a quiet location and dimming the lights. Skin to skin (kangaroo care) is also a good idea to help calm your baby.
What should I do if my baby is still on strike from breastfeeding?
– Track your baby’s wet and dirty diapers to make sure your baby is staying hydrated and getting enough substance. See “How Do I know My Baby is Getting Enough Breast Milk?”
– Keep offering your breast to the baby every three hours, even if you need to wake the baby.
– To avoid engorgement or plugged ducts, express your breast milk at the same time your baby would normally feed. You may feed your baby the expressed milk using a “cup, dropper, or spoon” (women’shealth.gov) these techniques are advised over bottles for exclusive breastfed babies.
Over Production of Breast Milk Say what? The more milk the better right? Not right. Too much breast milk can cause an overactive let-down, or in other words, a forceful milk ejection (picture a dog trying to drink from the garden hose on full blast). …
Breastfeeding moms may face a couple road bumps on their breastfeeding voyage. Breastfeeding can be difficult, awkward, messy, tiring, and not as simplistic and flawless as some pictures portray. Yet, the way a woman’s body is made to sustain another life is GLORIOUS! Not to …







{kind=link}
{kind=link}